“Airway is the reason that many go into emergency medicine…”
- Jaime McCarthy MD, UT Health Sciences Center at Houston EM Director
One of the many things that we do better than anyone in the business is obtain the emergent airway. Unlike our colleagues in other disciplines, we do not have the luxury of planning our airway approach on the golf course the evening before; we meet patients on their worst day. Even though we would often prefer it, we do not have the option to reschedule our intubations.
Smashed, bloody, distorted, edematous, airways secondary to trauma, anaphylaxis and GI bleeds are the things that we deal with routinely with nary a complaint or even a hither for a better look than what were given. We often feel lucky to get any type of view that resembles normal laryngeal anatomy. Personally, if I knew that I would need to be intubated today, that my airway would be bloody and edematous, and there was only time for one person to take a shot at placing the tube, then I would pray to God that the last face I see before the Roc and Etomidate push me asunder is the familiar grill of one of my EM colleagues. Who better to bet all my chips on then someone who deals with the hardest airways on the face of the planet as part of their daily routine? The general EM provider can not only get that airway, but is so relaxed about it that they will casually check on the patient in the next bed before and after the intubation. That’s the confidence I’m looking for when it comes to the fast paced life and death world of emergency airway.
Whether it is pediatric or adult emergency medicine, the most important thing that we do as “emergentologists and resusitologists” is control the airway.
iTunes Link
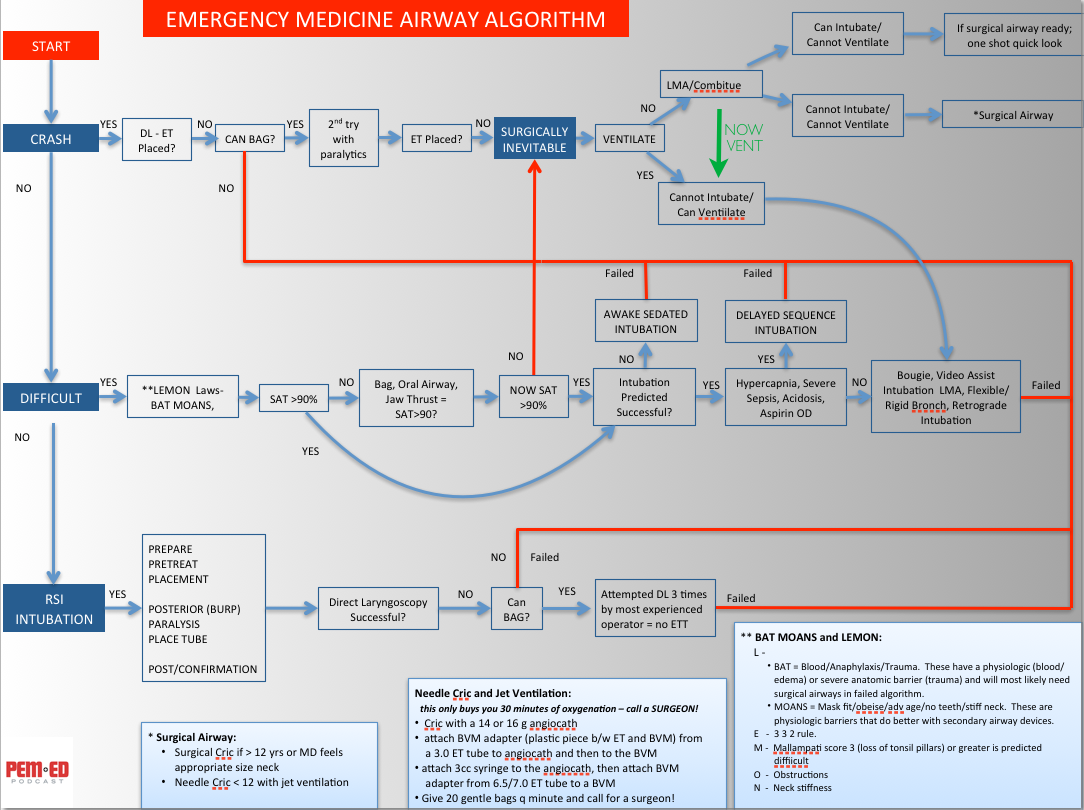
Mac Friendly Airway Algorithm
Podcast 6 - Pediatric Airway 101









{kind=link}
{kind=link}